EHS Secretary General, Professor Eleftherios Tsiridis
 COVID-19 cases are still rife around the world, with only the places that went for a zero-COVID strategy faring quite well now (such as Japan, Australia and New Zealand). Many countries in Europe have stopped elective orthopaedic surgery while the hospitals focus all staff on the critical COVID patients. Global deaths from the virus have passed 1.7 million and we can only be patient and wait for the vaccinations to be given.
COVID-19 cases are still rife around the world, with only the places that went for a zero-COVID strategy faring quite well now (such as Japan, Australia and New Zealand). Many countries in Europe have stopped elective orthopaedic surgery while the hospitals focus all staff on the critical COVID patients. Global deaths from the virus have passed 1.7 million and we can only be patient and wait for the vaccinations to be given.
This Month, our report is from Past President of EFORT and esteemed EHS member from Denmark, Prof Per Kjaersgaard-Andersen. Thank you very much to him. We also present two COVID-related articles from Prof Luigi Zagra (EHS SciCom) on OR efficiency and changes in clinical activity.
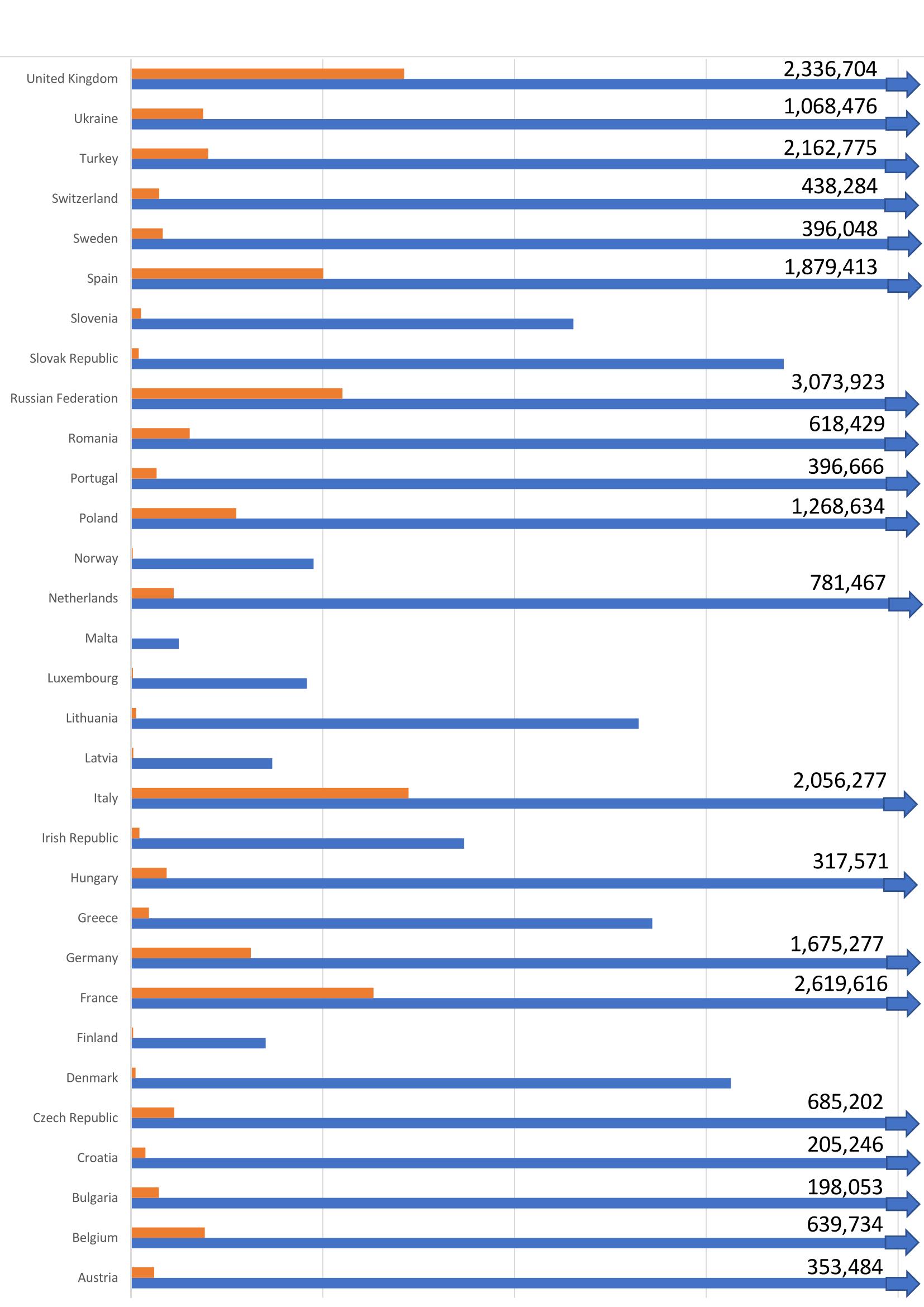
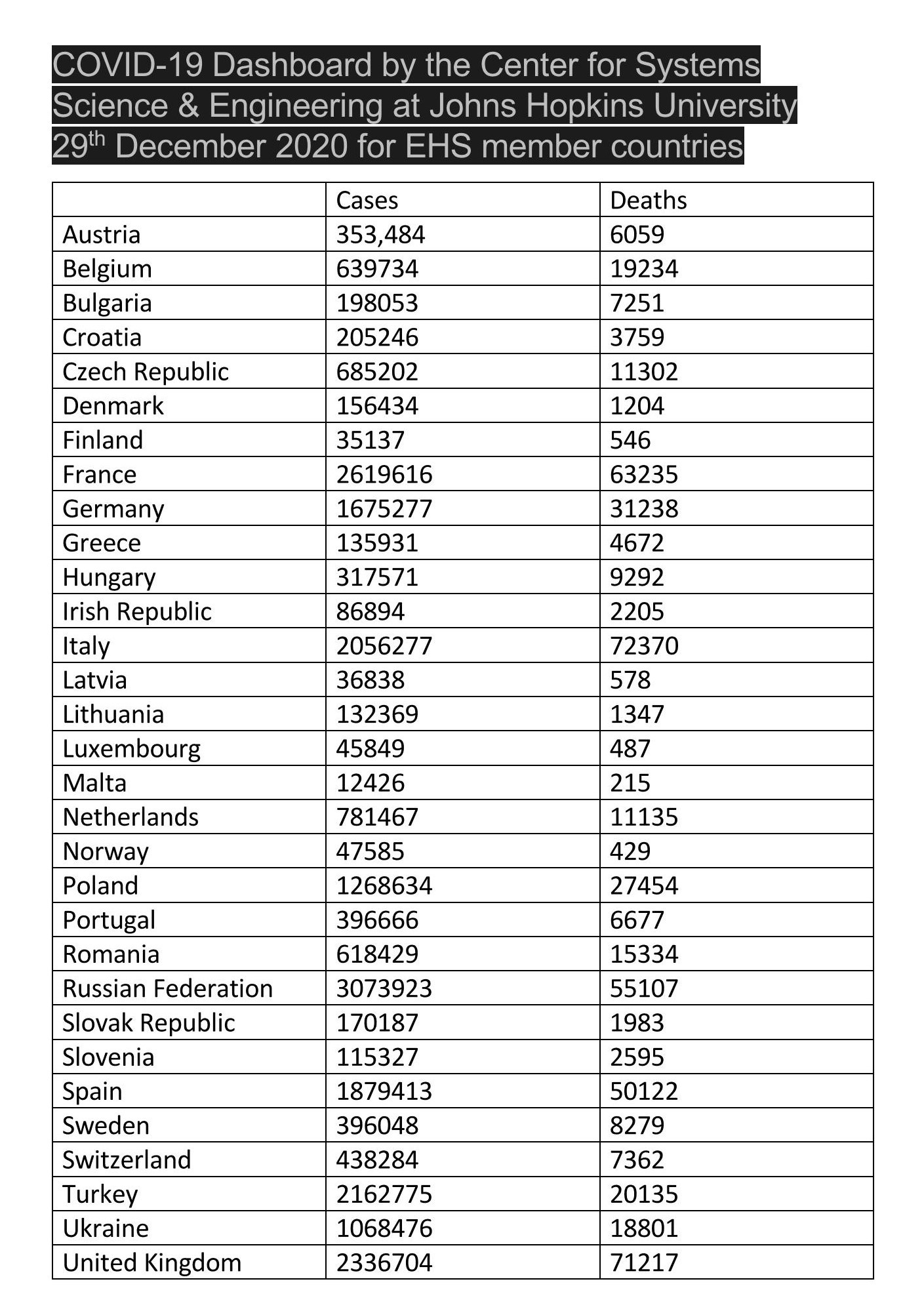
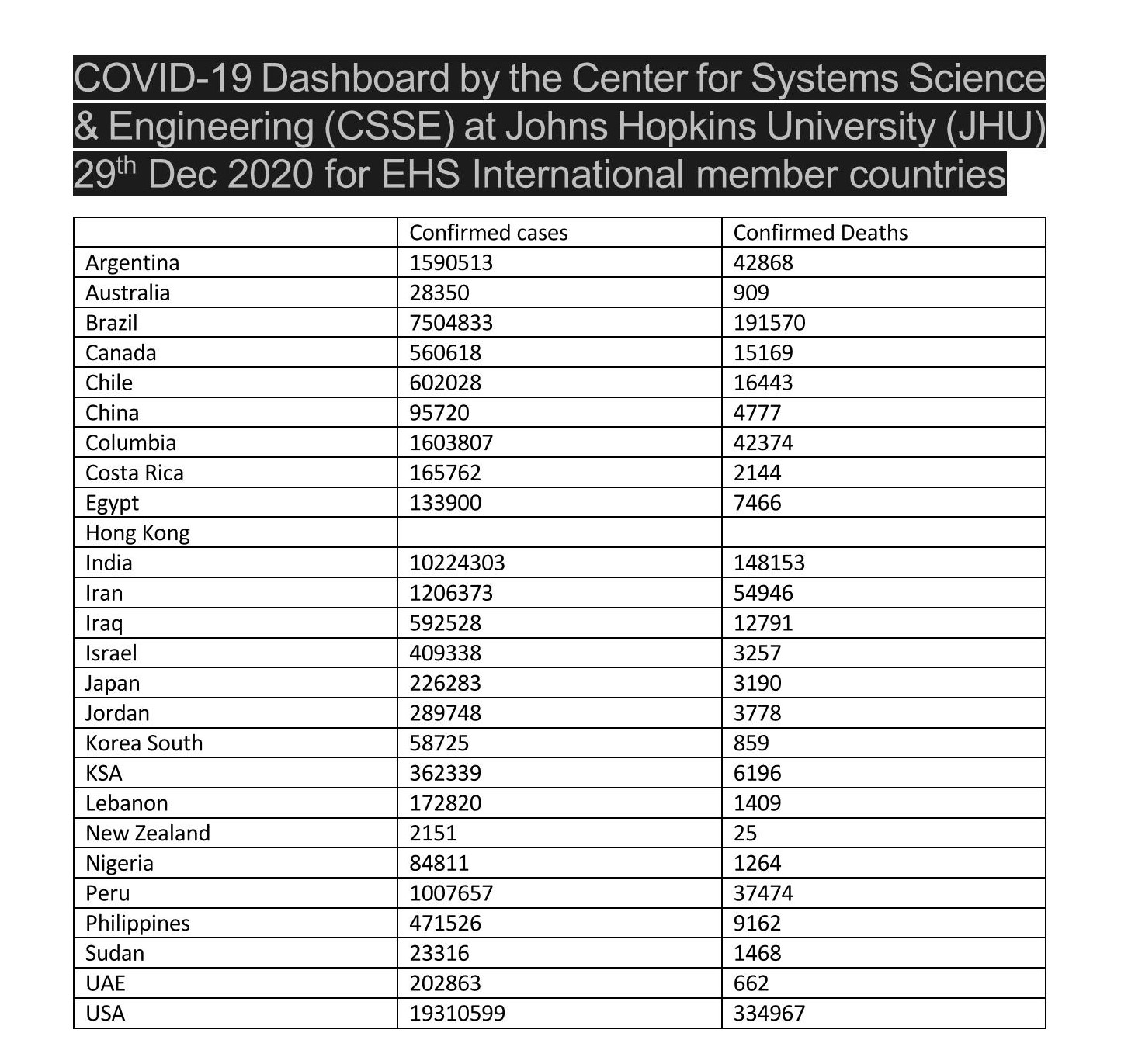
Finally we summarize the Johns Hopkins University data – as we do each month – for COVID-19 in our member countries, both in Europe and Internationally.
Please contact the EHS Secretarial Office via our Membership Secretary (samstokesehs@gmail.com) with reports on the COVID-19 developments in your area which you would like to share directly with our fellow hip surgeon members. Thank you.
COVID-Experience of a hip surgeon in Denmark, by Per Kjaersgaard-Andersen
 Dear colleagues,
Dear colleagues,
In Denmark we heard, like the rest of Europe, about the “new virus” in January 2020. A certain and natural alertness was given to this by both the media and also National Health Authorities. The latter quickly informed us that it would be very unlikely that this virus would reach Denmark – it would be handled and isolated in Asia.
A few weeks later, the same authorities warned of a possible pandemic also affecting Denmark, and after the first few cases had been identified in our country in early March, all with connection to ski resorts in Italy and Austria, the government overnight on March 11th demanded a total lockdown of our country.
The virus was now named Covid-19. Several regulations were sent out by the government in next days. Hospitals were reorganized to handle a possible high number of Covid-19 cases. All planned surgery, including joint replacement, was put on hold, outpatient clinics were closed down and factually only acute cases were taken in for surgery (infections, peri-prosthetic fractures, dislocations). Most orthopaedic departments across the country were reorganized to handle other types of patients. In my clinic at Vejle Hospital we were reorganized to handle patients with internal medicine diseases, under supervision of nurses and medical specialist from the department of medicine. Nurses in the OR-section and out-patients clinics were transmitted to other sections in the hospital, even some persons were asked to work now at other hospitals. Several health related persons were sent home on full salary, waiting for their need or replacement of sick colleagues.
The epidemic did also unfold in Denmark, but compared to most of Europe, our country had a very limited impact, although numbers of patients in ventilators and dying with Covid-19 rose exponentially for 2-3 weeks in April.
Probably due to the extreme national lock down, but also a significant fear among the citizens of becoming ill, the curve changed in late April early May, allowing the government to open the country stepwise from early June.
All departments of orthopaedics had postponed planned hip replacement for about 8-10 weeks, and only a few clinics were able to run at full capacity from early June. It has been calculated that approximately 12% of the expected annual THA procedures were cancelled / postponed. Individual initiatives to overcome the postponed cases were planned, including extra cases on the daily programme, surgery on Saturday and Sunday, and referral of public patients to private clinics. We are all still working on it, but will not be able to do same number of cases in 2020 as planned.
And now we are all on our way into the second wave of the pandemic. Severe precautions are taken to interview and test patients visiting the clinic for either examination or surgery, to prevent cases with Covid-19 to enter the clinic. This works nicely, although you cannot set-up a 100% safe procedure. Also, employees may bring the virus into the clinic, and currently we have regularly employees either home with Covid-19 or isolated at home waiting to be tested.
At same time the number of hospitalized patients with Covid-19 is rising again, but not to the same speed and amount as in the spring. This already now impacts some orthopaedic departments, again taking care of other types of patients than orthopaedics – and again cancelling planed THA cases.
Time has changed significantly, and we will be faced with this situation for yet several months until 60-70% of the population has been immunized by the upcoming vaccination.
Keep cool and stay safe,
Per Kjaersgaard-Andersen
EHS Member, EFORT President 2018-2019
Operating room efficiency and timing during coronavirus disease 2019 outbreak in a referral orthopaedic hospital in Northern Italy
- https://doi.org/10.1007/s00264-020-04772-x
Changes of clinical activities in an orthopaedic institute in North Italy during the spread of COVID-19 pandemic: a seven-week observational analysis
Luigi Zagra, Martina Faraldi, Fabrizio Pregliasco, Anna Vinci & Giovanni Lombardi