EHS Secretary General, Professor Eleftherios Tsiridis
 Summertime has inevitably increased COVID-19 cases worldwide and many popular holiday destinations now insist on the wearing of masks, even outdoors. Some cities have gone back into Lockdown, while a few countries are thinking of closing their borders again. Meanwhile, Oxford is at the last stages of making the vaccine available internationally and the EU and other governments are arranging for its fair distribution to all citizens.
Summertime has inevitably increased COVID-19 cases worldwide and many popular holiday destinations now insist on the wearing of masks, even outdoors. Some cities have gone back into Lockdown, while a few countries are thinking of closing their borders again. Meanwhile, Oxford is at the last stages of making the vaccine available internationally and the EU and other governments are arranging for its fair distribution to all citizens.
Below is an excellent report from our Nat Rep for Spain, Prof José Coredero-Ampuero, who reports from Madrid on his COVID-experience. Thank you to him. Following his thoughtful words, we summarise the Johns Hopkins University data as usual.
Please contact the EHS Secretarial Office via our Membership Secretary (samstokesehs@gmail.com) with any reports on the COVID-19 developments in your health care systems which you would like to share. With so much flooding of the media and the literature regards the pandemic, it is nice and refreshing to read some words directly from our fellow members.
COVID-Experience of a hip surgeon in Spain, by EHS Nat Rep for Spain, Prof José Cordero-Ampuero
 In the beginning of the first wave of COVID-19 (March 2020, 1st and 2nd weeks), the number of cases grew exponentially in Spain. Because of that, Spanish Health authorities stopped suddenly the programmed surgery from Monday March 16th. Waiting lists were absolutely blocked, and surgery was only allowed if it was actually urgent.
In the beginning of the first wave of COVID-19 (March 2020, 1st and 2nd weeks), the number of cases grew exponentially in Spain. Because of that, Spanish Health authorities stopped suddenly the programmed surgery from Monday March 16th. Waiting lists were absolutely blocked, and surgery was only allowed if it was actually urgent.
Why? The official reason was to avoid in-hospital transmission of virus. It was OK. A number of debilitated and/or very old patients, successfully operated of a periprosthetic or a trochanteric fracture, developed a COVID pneumonitis and died after a few days. Were they already infected when arriving to hospital? Were they contaminated inside the wards? Was the lengthened stay (families who did not assume after-hospital care) to blame?
But there was another essential reason: Intensive-care beds. Intensive-care units (ICUs) were beginning to collapse. Breathing-assistance machines were very scarce for the massive demand. And, more importantly, trained personnel to take care of those patients.
The Spanish Society of Intensive Care calculated that the total number of ICU beds were 6000 when adding public and private hospitals (for a total population of 47 million; meanwhile, Germany figures reached 13000 ICU beds for 80 million inhabitants). The urgent solution was straight: Post-surgical reanimation units were transformed in ICUs for COVID patients, surgical-theatre breathing machines were used for respiratory assistance in pneumonitis cases, and 1st and 2nd year surgical residents were used as UCI nurses.
All of us lived several hard experiences. Most of all, the terrible feeling of being useless. The lack of minimal knowledge, working blindly in the darkness of science. “Primum non nocere“, but, not acting at all? Or apply harmful actions? The fear about endurance of theatre-breathing machines: an ICU machine is devised and manufactured for working 24h/day along many uninterrupted days, but this is not the case for anesthetics machines. The social pressure (even when positive) and the demands from patients’ families. And, of course, fear about developing ourselves a severe illness.
We developed a lot of protocols or rules “on the move”. We had no time. We had to think fast and work directly, applying the classical “proof and mistake”. And we assumed continuously a lot of ethical doubts. Which dose of heparin for a COVID-positive hip fracture? When operate a trochanteric fracture with a pneumonitis? Treating conservatively subcapital fractures until hospital situation improved? No surgical treatment at all for any shoulder or wrist fracture? Send patients home only 48 hours after major surgeries?
Fortunately, although too slowly, validated protocols and guides were implemented. The whole hospital was divided in COVID positive and negative areas, including lobbies, aisles, wards, as well as theatres. Individual protection equipments (IPEs) were more and more available. Theatre-breathing machines were able to work perfectly and uninterruptedly along weeks. Surgical junior residents performed as well as UCIs nurses, they learned very fast, and supported adequately to our Anesthesiology colleagues. Older or risky staffs (over 50 approximately) were not allowed to participate in care of COVID patients. Everyday a special Surgical Committee gathered from 8.30 – 9.00 (after finishing the General Hospital Committee) to evaluate, decide and change whatever needed points or actuations. Those of us who got ill suffered generally a mild disease, and very few needed an ICU bed or, regrettably, died. Neither holidays nor vacations were allowed at all, even along Easter week.

And what was the specific activity of us, hip-specialized orthopaedic surgeons? Main dedication of those under 50 and COVID-free was helping our colleagues in Internal Medicine wards: About half of them were ill and isolated at home, those working were absolutely saturated, and the assistance in bureaucratic tasks and communication with families was very helpful. Meanwhile, we maintained about half of our visits to outpatients in a geographically distant location, our “Peripheral External Offices”, which were COVID-free. And of course we performed surgeries. As previously explained, only urgent surgeries were allowed. So we dedicated to hip and periprosthetic fractures, closed reduction of THA dislocations, and acetabular fractures.
COVID-negative trochanteric fractures were operated as early as possible in a COVID-free theater, seated next day, sent home after 48 hours, and closely followed in peripheral external office. The same protocol was applied to the very few acetabular and periprosthetic fractures. Severe doubts appeared when these patients were COVID-positive: to fix these fractures was necessary to seat and mobilize them, but, when was anesthesia less risky? We discussed every individual patient with Geriatrics and Anesthesia colleagues, taking into consideration thorax CT findings, peripheral blood oxygen level, general situation, comorbidities, etc.
The most used protocol we applied in geriatric subcapital fractures is still debated. Along the most terrible period of hospital collapse (from middle of March to end of April) we managed them conservatively: we seated patients immediately and prescribed powerful analgesia, sent them home after 48 hours, and followed them in external office. When health situation improved, patients were re-evaluated to operate them with an arthroplasty on a delayed basis. Which are the final results of this therapeutic scheme? We are collecting all data to re-evaluate short-term and global mortality, functional (recovery of walking ability) results, and development of new pathologies. We also want to compare results obtained with those from one year before, when equivalent patients were operated as early as possible.
We have had many more doubts in relation to our specific cases along that terrific period of hospital collapse: What to do with a recurrent dislocation, repeated more than once or twice along the described period? Repeated closed reductions, or a definitive surgery? If a loosened and mobilized cup is associated with a dislocation, is it wise to exchange that cup in a patient treated with immunocompromising drugs? How long to maintain a periprosthetic fracture in-hospital after surgery?…
I am writing this on August 31st. Clearly we are beginning a 2nd wave of virus expansion in Spain. Hospitals are again getting worse, perhaps more slowly than in March. In fact, most of Madrid public hospitals have from 10% to 20% of their total beds occupied by COVID patients. Surgical Departments have again stopped programmed and waiting-list surgeries (nowadays hospital protocols establish this point when COVID patients occupy over 5% to 10% of total beds).
In front of this situation, we have again plenty of unanswered questions. Are patients younger? Will ICUs not collapse this time? Will hip and periprosthetic
fractures decrease as in 1st wave, or will they continue appearing in great number? Are protocols developed in March and April correct? Must we use them? As a hip surgeon, What ideas can I suggest, trying to help, improve and contribute to the common well-being?
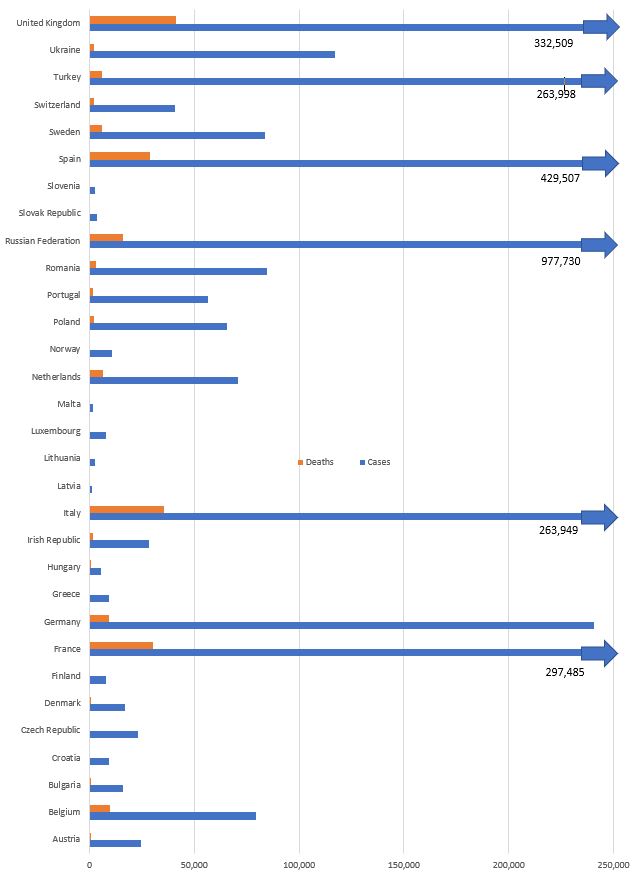
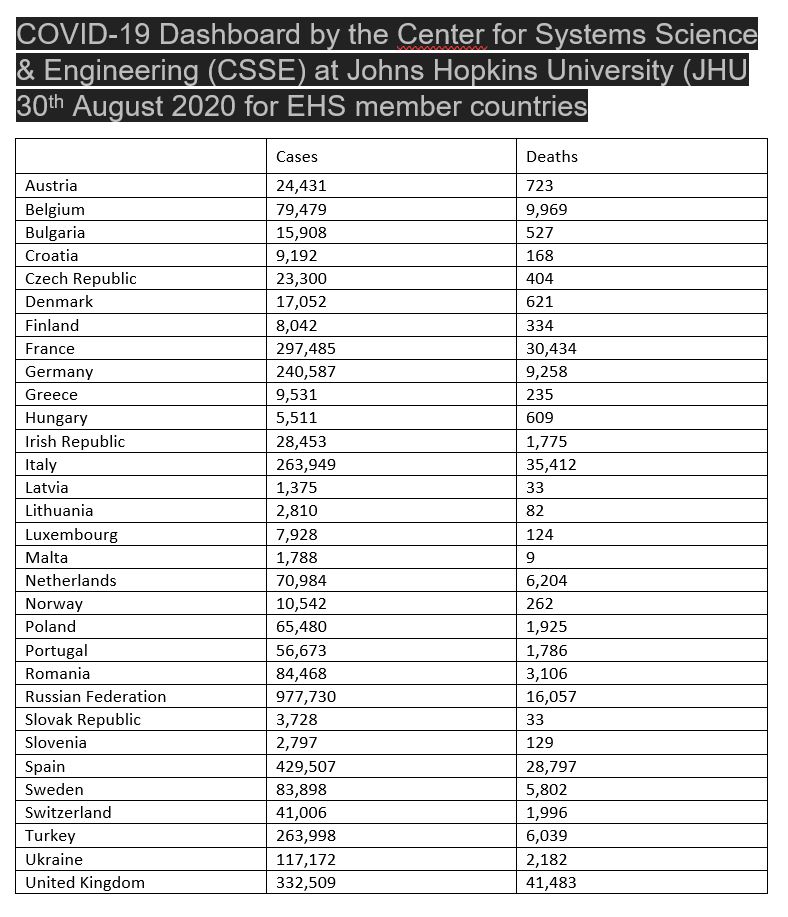
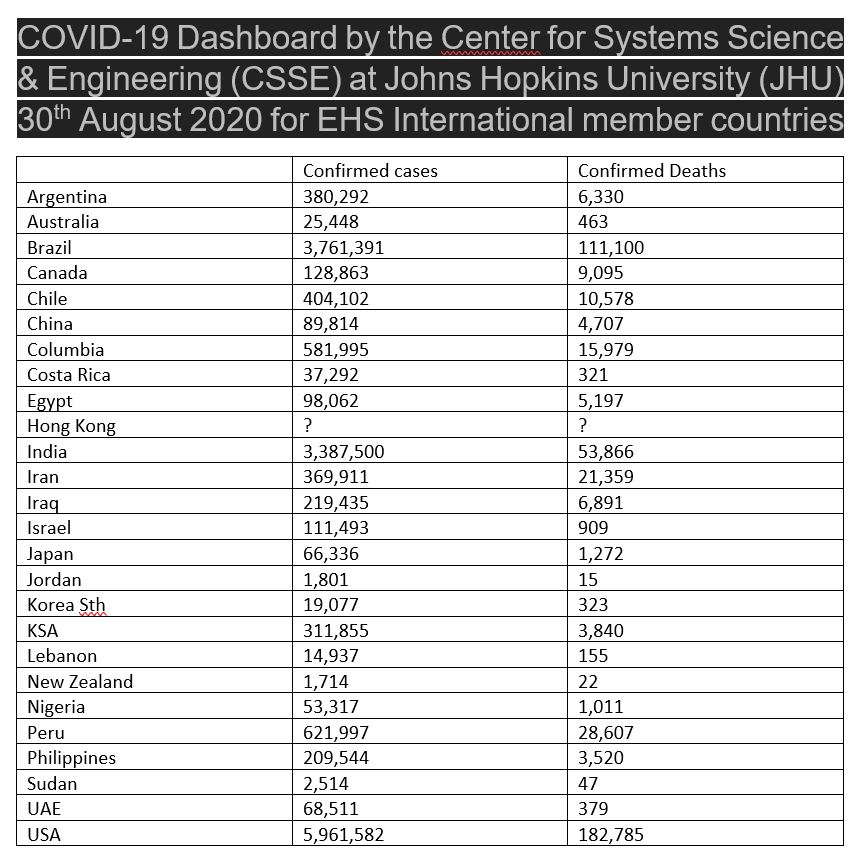
The latest figures for EHS member countries in Europe from the COVID-19 Dashboard by CSSE at Johns Hopkins University (JHU)