EHS Secretary General, Professor Eleftherios Tsiridis
EHS Secretary General, Professor Eleftherios Tsiridis
As orthopaedic surgeons return to elective work throughout Europe and the world, this page will link to international literature on the pandemic to help keep our community abreast of the virus. Please email your publications on Covid-19 to the EHS Secretariat Office (samstokesehs@gmail.com). We look forward to your contributions.
This month we feature a paper published by Prof Hart of the EHS EduCom with orthopaedic professors from Wuhan Hospital on: “Recommendations of protective measures for orthopedic surgeons during COVID-19 pandemic” (© ESSKA 2020).
Another article is by myself and three colleagues here in Greece on “Treating Patients With Primary Musculoskeletal Tumors in the Time of COVID-19 Pandemic, Alleviating the Pressure on Care-Providers” published now in CPQ Orthopaedics COVID Issue Paper.
Meanwhile, our Nat Rep for Belgium, Prof Thierry Scheerlinck, writes an excellent report from Brussels and beyond during the pandemic. Thanks to him.
Recommendations of protective measures for orthopedic surgeons during COVID‐19 pandemic
SPORTS TRAUMATOLOGY Published: 10 June 2020 / Knee Surg Sports Traumatol Arthrosc (2020).
Yulong Wang, Lian Zeng, Sheng Yao, Fengzhao Zhu, Chaozong Liu, Anna Di Laura, Johann Henckel, Zengwu Shao, Michael T Hirschmann, Alister Hart & Xiaodong Guo
Purpose: It was the primary purpose of the present systematic review to identify the optimal protection measures during COVID-19 pandemic and provide guidance of protective measures for orthopedic surgeons. The secondary purpose was to report the protection experience of an orthopedic trauma center in Wuhan, China during the pandemic.
Treating Patients With Primary Musculoskeletal Tumors in the Time of COVID-19 Pandemic, Alleviating the Pressure on Care-Providers
CPQ Orthopaedics COVID Issue Paper (Cient Periodique)
Papavasiliou Kyriakos, Prodoromos Hytiroglou, Christos Papandreou & Tsiridis Eleftherios* [*EHS Secretary General]
Due to the COVID-19 pandemic, most -if not all- elective orthopaedic surgery has been temporarily postponed worldwide. Patients with trauma and musculoskeletal tumors are generally excluded from this general rule. Nonetheless, during this COVID-19 outbreak, patients with primary benign and malignant tumors face the major risk of being unable to receive customary medical services in a timely fashion.
EHS Nat Rep for Belgium, Thierry Scheerlinck
 Brussels June 13th 2020
Brussels June 13th 2020
Dear colleagues,
Belgium is only a small country, but with 11.46 million inhabitants it is densely populated. As such, starting somewhere in the beginning of March, the sars-cov-2 could spread exponentially in all regions. With ±60,000 cases of COVID-19 and almost 10,000 deaths, Belgium has been severely impacted. The “lockdown” started on March 14th and although people were still authorised to leave their home, only “essential” trips were allowed. As in most European countries, the economy suffered harshly as “non-essential” industrial and service sectors were shut down or had to rely on “homeworking”.
Health care in Belgium is well developed with ±6.19 hospital beds/1000 inhabitants (EU average 5.15) and rather few doctors and many nurses compared to the EU average. Most doctors are self-employed and rely on a pay-for-performance reimbursement system with a compulsory health insurance that is nearly universal. Based on the experience in Italy, and to avoid overcrowding, all hospitals went in a “lockdown” mode as from mid-March on. At that time less than 100 COVID-19 cases had been admitted, but all “non-essential” treatments and hospitalisations were postponed. The capacity of intensive care (IC) beds was maximized by converting operating theatres, recovery rooms and mid-care units. As such, by March 22nd, the minister of health announced that 759 extra IC beds had been provided. For this, the total IC capacity reached 2650 beds in Belgium. Patient’s flows in the emergency room were divided in non-COVID, unknown-COVID and COVID areas. All incoming patients were screened by pulmonary CT scan as this was perceived as the fastest and most reliable test, followed by standard PCR with results within 12 to 24 hours. This was later often replaced by fast PCR that was not available at that time. Wards were allocated to the treatment of COVID and non-COVID patients. Nurses, trainees and internal medicine doctors were trained to care for COVID patients, but in most cases orthopaedic surgeons were not involved except for the screening of patients in some hospitals. Overall, these measures were successful as the combination of a lockdown of the population, freeing of hospitalisation capacity in an early stage and increasing the number of IC beds kept the crisis in most hospitals under control. However, we suffered a high global mortality rate in Belgium. This was attributed, at least partially, to outbreaks in residential care centres that accounted for almost half the dead due to COVID or suspected COVID.
For the orthopaedic (hip) surgeon the COVID crisis meant basically that only trauma cases, infections and malignant tumours were operated on and that, whenever possible, conservative treatment was favoured. In contrast to what was reported in Italy by the EHS national representative Nicolas Santori, cases were not concentrated in few selected centres, but all orthopaedic departments continued to operate throughout the crisis, be it a very low rate. As such, most orthopaedic surgeons operated only few cases, but stayed in stand-by. Actually, the health system was never under very high strain and at the height of the crisis only half the extended IC capacity (2650 beds) was in use. The vast majority of hospitals in Belgium have a mix of private and public patients, private patients being admitted in single rooms and non-private in double rooms. As such, there was no need for a close collaboration between the private and public sector and we did not experience a real shortage of hospital beds.
Although orthopaedic surgeons did not in general look back at the Corona crisis as a catastrophe from a medical point of view, many experienced it as a major economic problem. Indeed our health system, that generally performs very well, is based on self-employed doctors and on a pay-for-performance reimbursement system. As such, there was no good solution for doctors that were not allowed to operate or were temporarily employed in Intensive Care or Emergency departments. The only exceptions were doctors employed in academic hospitals. They kept a fixed income and enjoyed some spare-time to do research, to record lectures for online courses and to prepare for exams keeping social distancing in mind. As such, starting May 18th when the crisis eased and surgeons were allowed to see outpatients beside emergencies and to operate elective cases, doctors were very keen to resume their normal duties. Although politicians did not impose strict rules to do this, most centres resumed very progressively their outpatient clinics, spreading patients over larger periods of time to avoid crowded waiting rooms and increasing opening hours to provide enough capacity. As operating theatre nurses were released from Intensive Care and COVID units, normal OR activities could be resumed gradually.
Now many centres operate almost as before the crisis and outpatient clinics have resumed about 80% or more of their pre-Corona activities. Most hospitals are now “Corona-free” as the total number of COVID-hospitalisations in Belgium decreased to 425 from a maximum of almost 6,000 cases in mid-April. At this time, the only remains of the crisis are the face masks that are now worn throughout the hospital, the social distancing rules that prevent large face-to-face meetings and a new way to greet patients and colleagues… I believe it is only once hand-shaking will be back again, that we will all be relieved that the Corona crisis has finally been fully dealt with.
Your sincerely,
Thierry Scheerlinck
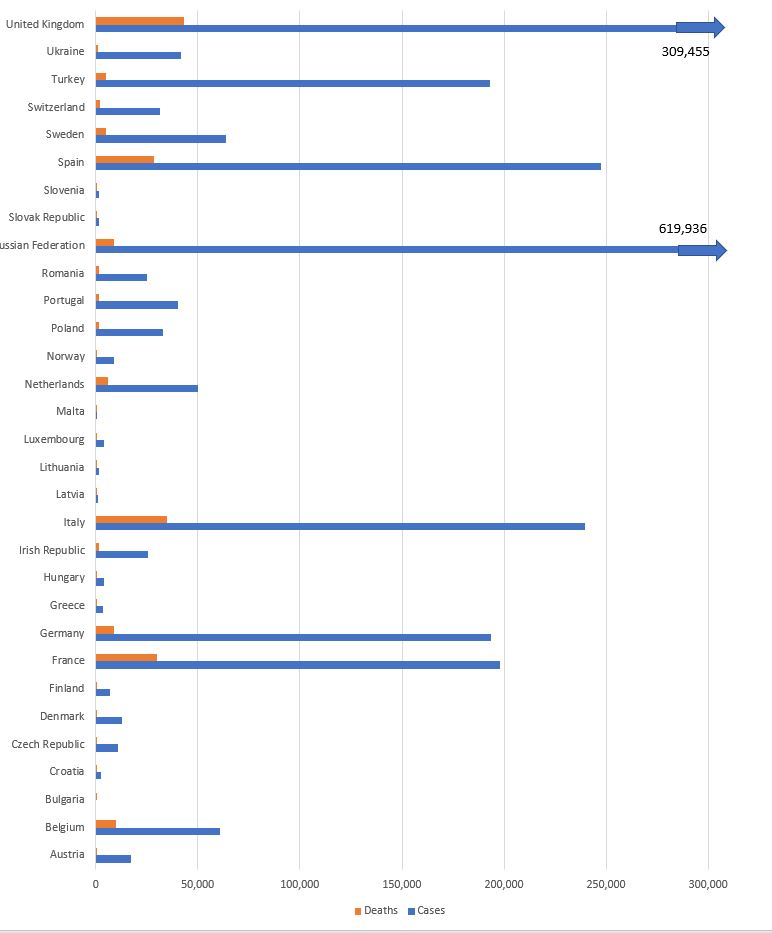
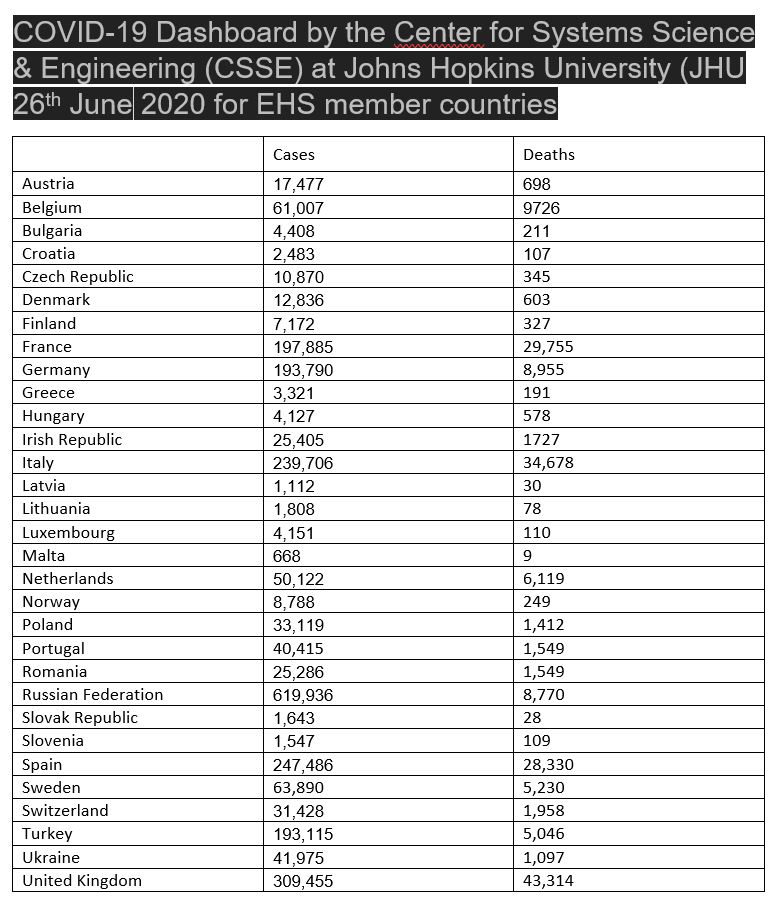
The latest figures for EHS member countries in Europe from the COVID-19 Dashboard by CSSE at Johns Hopkins University (JHU)