EHS Secretary General, Professor Eleftherios Tsiridis
 Last month, there had been 33 million cases of COVID-19 worldwide. This month there have been 43 million. The numbers keep rising, and in the media we read words like spike and surge, but a vaccine is ever closer and some good results have come out of UK this week, including findings of a robust antibody and T-cell immune response in volunteers aged 56 and over, as announced by Professor Andrew J Pollard, the chief investigator of the global clinical trials of the Oxford COVID-19 vaccine sponsored by the University of Oxford.
Last month, there had been 33 million cases of COVID-19 worldwide. This month there have been 43 million. The numbers keep rising, and in the media we read words like spike and surge, but a vaccine is ever closer and some good results have come out of UK this week, including findings of a robust antibody and T-cell immune response in volunteers aged 56 and over, as announced by Professor Andrew J Pollard, the chief investigator of the global clinical trials of the Oxford COVID-19 vaccine sponsored by the University of Oxford.
Members of the European Hip Society all abide by different levels of restrictions, according to our country’s cases and our government’s reactions. This month we hear from our Nat Rep for The Netherlands, Dr Stephan Vehmeijer on what the current situation is there – thanks to him or his Covid-19 report below. In October we heard from Australia, and prior to that Spain, USA, Belgium, Italy and Switzerland.
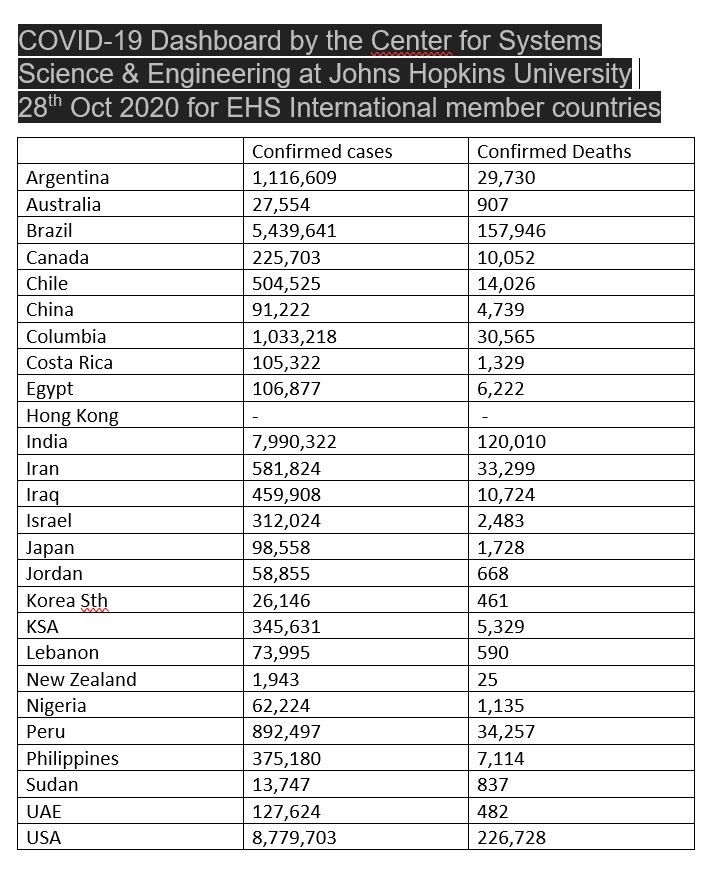
Following this, we summarise the Johns Hopkins University data.
Please contact the EHS Secretarial Office via our Membership Secretary (samstokesehs@gmail.com) with reports on the COVID-19 developments in your area which you would like to share directly with our fellow hip surgeon members.
COVID-Experience of a hip surgeon in The Netherlands, by EHS Nat Rep, Dr Stephan Vehmeijer

Dear colleagues,
The first reports of the European spread of Covid-19 came from the Northern provinces of Italy. A colleague in Bergamo told me frightening stories of overcrowded hospital wards and IC units. Orthopedic surgery was restricted to trauma surgery only. Several of his colleagues were infected by Covid-19. In the meantime we prepared ourselves in our hospitals and hoped the same scenario would not happen in The Netherlands.
By the end of February 2020, however, COVID-19 reached the South of the Netherlands and also resulted in massive hospitalization of patients both on the ward and the IC units. By the end of March most hospitals reached their maximum ICU capacity and patients even had to be transferred to German hospitals that very generously welcomed them to their care.
In our country all the elective surgery, including all elective orthopedic surgery, came to a full stop in the second half of March. Many surgeons were asked to help in different departments of their hospitals, including the emergency department and at the COVID wards as a help for e.g. the lung physicians. Everybody helped in their own way to overcome this health care crisis. For instance, private clinics (ZBC’s) made their ventilators and nursing staff available to hospitals and donated their surgical masks and gowns to clinics that needed these desperately due to the shortage of protective materials.
By the end of April, after a limited lockdown, the number of new infections, hospital admissions and deaths due to the Corona virus decreased to a point where elective surgery was possible again under strict circumstances.
From webinars organized by our National Orthopedic Society (NOV) it became clear that it was safe to perform surgery without a pre-operative COVID-19 test or CT-scan on patients without signs of COVID. In the Netherlands, throughout the summer the number of infections remained low, which enabled us to partially catch up with the lag in patients waiting for surgery prior to and during the lockdown.
Unfortunately earlier than expected the second wave has started and currently hospitals are again flooded with COVID-19 patients. Unlike the first wave, due to the improved treatment and the relative young age of the infected patients, the ICU capacity is not a problem yet. This time, mainly the hospital wards are overloaded with COVID-19 patients. Also a shortage of nursing staff due to sickness or suspected Corona infection have resulted in a decreased number of available beds.
We have learned from the first wave when mainly hospitals in the South of the country were overcrowded. This time we actively distribute the Covid-19 patients evenly over the whole country, in order to maintain a percentage of elective surgery in each hospital. Again, despite these efforts, the number of orthopedic surgical procedures is reduced while personally I still have patients from prior to the first wave on my list.
Unfortunately the general view of our other medical colleagues is that patients with for instance hip or knee arthritis can easily wait a few extra months for their treatment. Some patients may be forced to wait for a whole year before their surgery can take place. The effect of the reduced mobility and their pain on daily life should not be underestimated. Hopefully we can help these patients soon, but I’m afraid it’s going to be a long winter.
Stay safe,
Stephan Vehmeijer
National Representative for the Netherlands
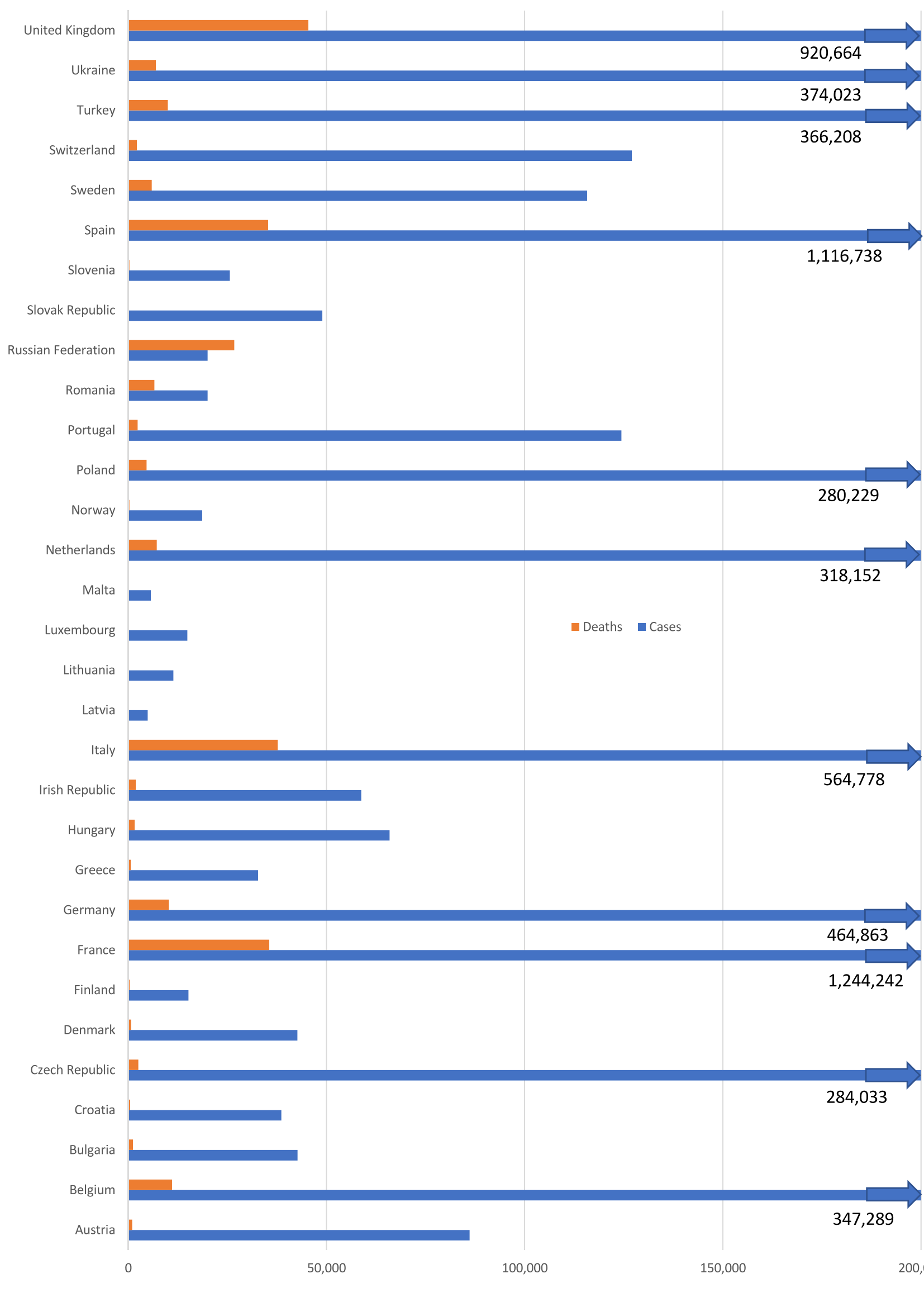
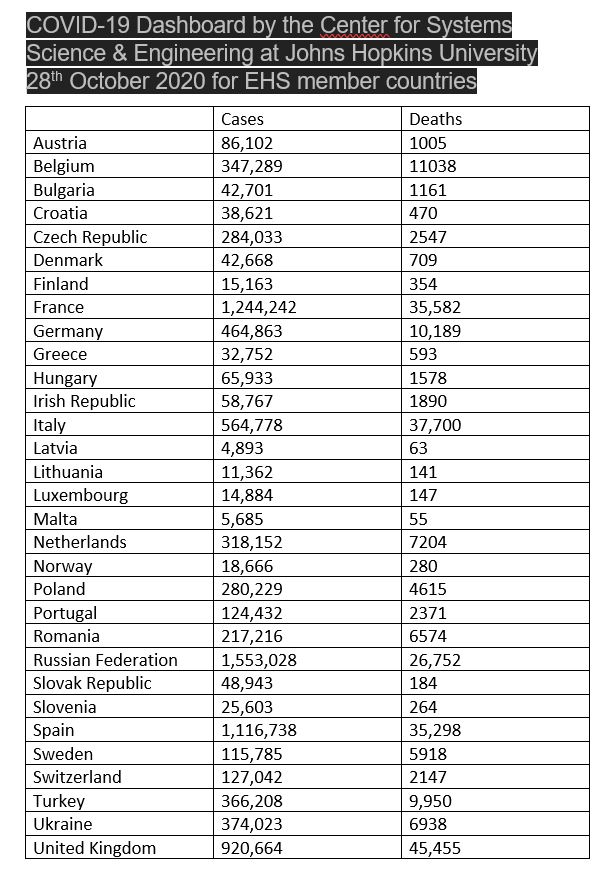
The latest figures for EHS member countries in Europe from the COVID-19 Dashboard by CSSE at Johns Hopkins University (JHU)